Helen O Ogefere1 ![]() ,
James G Osikobia1,
Richard Omoregie2,3
,
James G Osikobia1,
Richard Omoregie2,3
For correspondence:- Helen Ogefere Email: helenogefere@yahoo.com
Received: 23 January 2016 Accepted: 7 June 2016 Published: 30 September 2016
Citation: Ogefere HO, Osikobia JG, Omoregie R. Prevalence of AmpC ß-lactamase among Gram-negative bacteria recovered from clinical specimens in Benin City, Nigeria. Trop J Pharm Res 2016; 15(9):1947-1953 doi: 10.4314/tjpr.v15i9.20
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: Infections caused by AmpC-positive bacteria results in high patient morbidity and mortality making their detection clinically important as they cannot be detected in routine susceptibility testing. This study aim to determine the prevalence of AmpC β-lactamase among Gram negative bacteria recovered from clinical specimens in Benin City, Nigeria.
Methods: A total of 256 consecutive and non-repetitive Gram negative bacteria were recovered from various clinical specimens. The prevalence of AmpC β-lactamase was determined using a combination of disc antagonism test and cefoxitin-cloxacillin inhibition test. Disc susceptibility test was performed on all isolates using standard techniques.
Results: Cefoxitin-cloxacillin inhibition test detected more AmpC β-lactamase than other tests. The prevalence of AmpC β-lactamase did not differ significantly between both genders and between in-patients and out-patients (p>0.05). Isolates recovered from sputum had significantly higher prevalence of AmpC β-lactamase producers compared with isolates from other clinical specimens (p=0.0484). The prevalence of AmpC production was significantly higher among isolates of Pseudomonas aeruginosa than other isolates (p = 0.0085). Isolates that produced AmpC β-lactamase were more susceptible to the test cephalosoprins.
Conclusion: An overall prevalence of AmpC β-lactamase (15.23 %) was observed in this study. Pseudomonas aeruginosa was the most prevalent producer of AmpC enzymes. Prudent use of antibiotics is advocated.
Introduction
Drug and multidrug resistant bacterial pathogens that are causative agents of infectious disease constitute a serious public health concern [1]. The development of new antibiotics has been accompanied by the steady increase of antibiotic-resistant bacterial strains and the diversity of mechanisms used by bacteria to surpass the lethal effect of these compounds [2]. Many bacterial species show multi- or pan-resistant phenotypes and most of these multidrug resistant (MDR) bacteria can cause life-threatening infections, and are of major concerns both in the hospital and the community [3,4]. The prevalence of multidrug-resistant Gram-negative bacteria has increased continuously over the past few years [5].
Beta lactam antibiotics are still the most predominantly prescribed antibiotics to treat bacterial infections, especially in Nigeria hospitals [6,7]. Over the last two decades many new β-lactams have been developed that were specifically designed to be resistant to hydrolytic actions of β-lactamases [8]. But a new type of β-lactamase such as AmpC β-lactamase has emerged [8]. AmpC β-lactamases are class C or group I cephalosporinases that confer resistance to a wide variety of β-lactam antibiotics including penicillins, cephalosporins, oxyimino-cephalosporins (e.g., ceftriaxone, cefotaxime, and ceftazidime), cephamycins (e.g., cefoxitin and cefotetan), and monobactams (aztreonam). The activity of this enzyme is not affected by the ESBL inhibitor clavulanic acid, sulbactam and tazobactam [5,9-11]. Infections caused by AmpC-positive bacteria are therefore of particular clinical and epidemiological importance and as they cause higher patient morbidity and mortality [12]. Indeed, mortality rates of 14.3 – 46 % have been reported [13]. AmpC β-lactamases are not detected in routine susceptibility test and are typically associated with multiple antibiotic resistances, leaving few therapeutic options [14-16]. Therefore, detecting AmpC-positive bacteria is clinically important, not just because of their broader cephalosporin resistance, but also because carbapenem resistance can arise in such strains by further mutations, resulting in reduced porin expression as well as false positive extended spectrum β-lactamase screening test [5,17]. Against this background and lack of data on the prevalence of AmpC β-lactamase in Benin City, Nigeria, this study was conducted to determine the prevalence of AmpC β-lactamase among Gram negative bacterial recovered from clinical specimens. The susceptibility profiles of AmpC-positive and AmpC-negative bacteria will also be determined.
Methods
Bacterial isolates
A total of 256 consecutive non–repetitive bacterial isolates recovered from various clinical specimens from patients attending University of Benin Teaching Hospital, Benin City (UBTH), Benin City, Nigeria, were used for this study. The isolates included Escherichia coli, Klebsiella species, Citrobacter species, Proteus species, Providencia species, Acinetobacter species, Alcaligenes species and Pseudomonas aeruginosa. All isolates were identified using standard techniques [18].
Detection of AmpC β-lactamase
The presence of AmpC β-lactamase was detected by the combination of the methods of Livermore and Brown [19] and Peter-Getzlaff et al [20]. Briefly, test organisms were emulsified in sterile water and the turbidity matched with 0.5 McFarland standards. Once matched, a sterile cotton wool swab was dipped in the organism suspension and excess liquid was removed by turning the swab on side of the test tube. The entire surface of Mueller–Hinton agar plate was seeded by swabbing in three directions with the swab. A 30 µg cefoxitin disc was placed on the seeded plated and flanked on either side by a 30 µg ceftazidime and a 30 µg ceftriaxone discs placed 15 mm from the cefoxitin disc. Another 30 µg cefoxitin disc supplemented with 200 µg cloxacillin was placed in another area of the seeded plate. The plates were incubated at 37 oC overnight. AmpC production is inferred if there was blunting or flattening of the zone of inhibition of either the ceftazidime or ceftriaxone or both [disc antagonism test (DAT), 19]. Comparing the zone diameters of the cefoxitin discs with and without cloxacillin infers AmpC β-lactamase production if the difference in the zone diameters is ≥4 mm [cefoxitin-cloxacillin inhibition test (CCIT), 20]. An isolate that is positive for the disc antagonism test or the cefoxitin-cloxacillin inhibition test or both was considered positive AmpC β-lactamase.
Disc susceptibility testing
Disc susceptibility tests were performed on all bacterial isolates using the British Society for Antimicrobial Chemotherapy (BSAC) method [21].
Statistical analysis
The DAT method detects chromosomal-mediated AmpC production while the CCIT method detects plasmid-mediated AmpC production. Prevalence of AmpC was determined by adding AmpC producers detected by DAT alone, CCIT alone and where both methods detected AmpC in an isolate. The total number was expressed as a percentage of 256. The data obtained were analyzed with Chi square (X2) test and odds ratio analysis using the statistical software INSTAT® (Graph Pad Software Inc, La Jolla, CA, USA). Statistical significance was set at p < 0.05.
Results
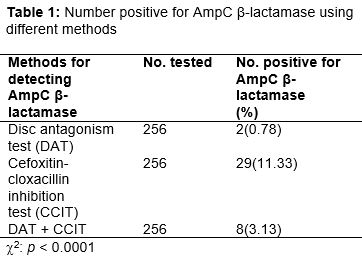
A total of 39 (15.23 %) out of the 256 Gram negative bacterial isolates were positive for AmpC β-lactamase. Of these isolates that were positive for AmpC β-lactamase, the disc antagonism test detected 2 (0.78 %), the cefoxitin-cloxacillin inhibition test detected 29 (11.33 %) while 8 (3.13 %) were detected by both methods, and the difference was statistically (p < 0.0001) significant ().
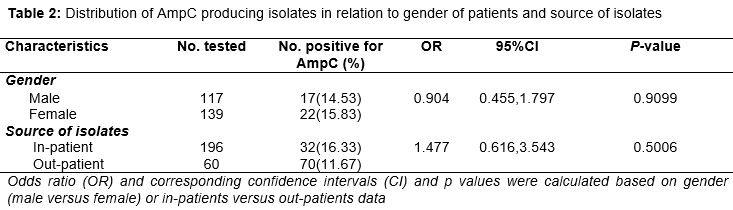
The distribution of AmpC producing Gram negative bacterial isolates in relation to gender of patients and source of isolates is shown in . The prevalence of AmpC β-lactamase did not differ significantly (p = 0.9099) between isolates recovered from males (14.53 %) and those recovered from females (15.83 %). The prevalence of AmpC production was higher among isolates recovered from in-patients (16.33 %) compared with those recovered from out-patients (11.67 %) and isolates from in-patients were associated with AmpC production (OR = 1.477, 95 %CI = 0.616, 3.543), although, it was not statistically significant (P = 0.5006).
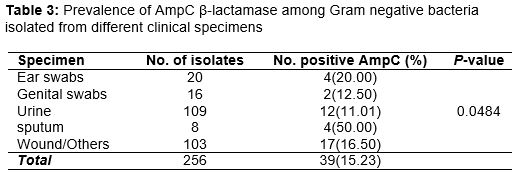
AmpC production was highest among isolates recovered from sputum (50.00 %) followed by isolates recovered from the ear (20.00 %) and the distribution of AmpC production differ significantly (p = 0.0484) between isolates recovered from various clinical specimens ().
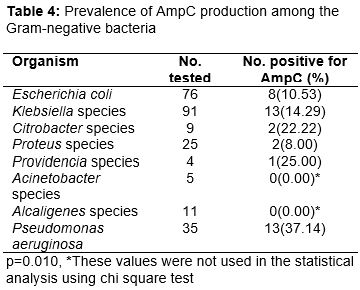
The prevalence of AmpC production among the Gram negative bacteria used in this study is shown in . Pseudomonas aeruginosa were the most prevalent producers of AmpC (37.14 %) followed by Providencia species. All strains of Acinetobacter species and Alcaligenes species used in this study did not produce AmpC β-lactamase. There was a significant difference in the prevalence of AmpC β-lactamase among the various genera of Gram negative bacteria used in this study (p = 0.0103).
The susceptibility profiles of AmpC-producing and non-producing Gram negative bacteria are shown in Tables 5 and 6 respectively. Generally, the susceptibility profiles ranged from poor to high depending on the isolates and the antibacterial agent and isolates that produced AmpC were more susceptible to the used antibacterial agents.
Discussion
Of the 256 Gram negative bacteria used for this study, DAT method detected 2(0.78 %) AmpC producers, CCIT method detected 29 (11.33 %) producers while both methods detected 8(3.13 %) AmpC producers simultaneously. Usually, AmpC β-lactamase are either plasmid-or chromosomal-mediated [5,12]. DAT detects chromosomally-mediated AmpC production [11,19] while CCIT detects plasmid-mediated AmpC production [12]. This indicates that both chromosomal and plasmid-mediated AmpC β-lactamase were present, though the prevalence of plasmid-mediated AmpC β-lactamase was significantly higher (p < 0.0001). This is worrisome as this mode of resistance can easily be transferred among Gram negative bacteria. It has been reported that such plasmids can harbour high number of resistant genes associated with carbapenem resistance, ESBL genes, aminoglycoside resistant genes, macrolide resistant genes, rifampin and sulfamethoxazole resistance genes as a source of multi-drug resistance [22,23]. This limits therapeutic options. Chromosomal-mediated AmpC β-lactamases are inducible and such isolates are resistant but produce small amounts AmpC β-lactamase [5,19]. However, AmpC-inducible species segregate derepressed mutants which produce their AmpC enzymes copiously without induction, and these mutants are resistant to almost all penicillins and cephalosporins [24,25]. Therefore, detection and differentiation of both chromosomal- and plasmid-mediated AmpC β-lactamase is essential.
The prevalence of AmpC β-lactamase in this study was 15.23 % (39/256). This is lower than the 31% and 37 % previously reported [13,26]. The difference could be due to geographical location or the manner in which the prevalence was determined. Black et al [13] study was conducted in the United States of America, Shivanna and Rao [26] study was conducted in India, while this study was conducted in Nigeria. In both Black et al [13] and Shivanna and Rao [26] study, the prevalence of AmpC β-lactamase were calculated from isolates resistant to cefoxitin while the prevalence of AmpC-positive in this study was calculated from the total isolates used. The prevalence of AmpC β-lactamase observed in this study was higher than that reported in Kano (2 %) [27]. This may indicate that regions within the same country may have different prevalence rates of AmpC-positive isolates, and this may reflect the degree of antibiotic abuse in the different regions of the country as antibiotics use is unregulated in Nigeria.
There was no significant difference in the prevalence of AmpC β-lactamase between isolates recovered from males and females (p = 0.9099). This agrees with the findings of Yusuf et al [27]. Similarly, there was no significant difference (p = 0.5006) in the prevalence of AmpC β-lactamase among isolates recovered from in-patients and out-patients.
A similar finding was recently reported in relation to ESBL in our institution [28]. Prior use of broad spectrum antibiotics such as β-lactam antibiotics (cephalosporins) are risk factors for ESBL [29,30]. Exposure to β-lactam antibiotics can result in AmpC β-lactamase production [31]. In Nigeria, extended-spectrum cephalosporins and fluoroquinolones are widely used as broad spectrum antibiotics and remain the drugs of choice to treat infections caused by various Gram negative pathogens [32]. This together with the unregulated use of antibiotics in Nigeria may explain this finding.
In this study isolates recovered from sputum had the highest prevalence of AmpC production. This is not in agreement with the findings of Yusuf et al [27] where isolates from urine were the predominant producers of AmpC β-lactamase. No reason could be adduced for this difference, albeit, the prevalence of AmpC β-lactamase differ significantly among Gram negative bacteria recovered from various clinical specimens (p = 0.0484).
The prevalence of AmpC β-lactamase differ significantly (p = 0.0103) among the genera of Gram negative bacteria with strains of Pseudomonas aeruginosa been the most prevalent producers of AmpC β-lactamases. AmpC β-lactamase has been reported to be chromosomally-mediated in Pseudomonas species [33]. However, strains of Pseudomonas aeruginosa harboured both chromosomal and plasmid-mediated AmpC β-lactamase. Strains of Acinetobacter species used in the study were negative for AmpC β-lactamase. However, other authors have reported Acinetobacter species as producers of AmpC β-lactamase [34]. Molecular studies are needed to verify this as they are seen as the gold standard in AmpC β-lactamase detection [33]. The susceptibility profiles of AmpC β-lactamase-producing Gram negative bacteria reveals poor to high activity with β-lactamase antibiotics.
AmpC producers have been reported to be susceptible to extended-spectrum cepholospo-rins in-vitro [35] but when these β-lactam drugs are used they result in treatment failure [20]. Therefore, these agents will not be useful in treating infections caused by these organisms. Ofloxacin was the most active agents against AmpC-producing Gram negative bacteria. Among the non-AmpC-producing Gram negative bacteria, the susceptibility profiles were generally poor, indicating higher level resistance, probably due to unregulated use of antibiotics and over the counter sales of antibiotics without prescription [36-38], and treatment of patients by clinician without recourse to laboratory guidance [39].
Conclusion
An overall prevalence of AmpC β-lactamase of 15.23 % has been observed in this study. Pseudomonas aeruginosa is the most prevalent producer of AmpC enzymes. Prudent use of antibiotics is recommended.
Declarations
Acknowledgement
References
Archives


News Updates